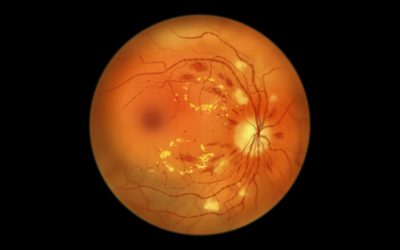
Diabetic macular edema affects an estimated 347 million people worldwide with diabetes, making it a leading cause of visual impairment that can steal your sight without warning. What makes this condition particularly concerning is its rapid progression: untreated DME causes more than half of patients to lose more than two lines of visual acuity within just 2 years.
Current treatments for diabetic macular edema have evolved dramatically beyond traditional approaches.
The good news is that current treatments for diabetic macular edema have evolved dramatically beyond traditional approaches. While laser therapy dominated treatment decisions for decades, accounting for nearly 85% of cases from 2009 to 2011, anti-VEGF medications have now emerged as the preferred first-line therapy. These advanced treatments can halt progression and often restore vision that seemed lost forever.
Your treatment options today extend far beyond what was available even a decade ago. Whether you’re facing a recent diagnosis or seeking better management of existing macular edema, understanding your choices helps you work effectively with your eye care team.
This guide explores many of the available treatments for diabetic macular edema to protect your vision, including cutting-edge medications, precise injection techniques, targeted laser procedures, and strategic combination approaches that can reduce treatment burden while maximizing results.
Current Treatments for Diabetic Macular Edema: Medication Options
Anti-VEGF medications: First-line treatment
Anti-vascular endothelial growth factor (anti-VEGF) therapies work by targeting VEGF, a troublesome protein that drives fluid leakage and abnormal blood vessel growth in diabetic macular edema. Think of VEGF molecules as keys that unlock blood vessel walls, allowing fluid to leak into your macula. Anti-VEGF medications work by binding to these molecular keys, preventing them from reaching the receptors on blood vessel walls.
When you receive these medications, they block VEGF-A molecules, reducing vascular permeability and retinal edema to stabilize and often improve your visual acuity. This targeted action stops the cascade of events that leads to vessel leakage and macular swelling.
Anti-VEGF injections have become the standard first-line treatment for the management of sight-threatening diabetic macular edema (DME).
Ranibizumab, Bevacizumab, and Aflibercept compared
The three primary anti-VEGF medications have distinct characteristics that may influence which one your doctor recommends.
Ranibizumab represents a recombinant monoclonal antibody fragment designed specifically for ocular use. The landmark RISE and RIDE studies revealed impressive results: over 40% of study patients receiving ranibizumab experienced 15 letters or more improvement in visual acuity, compared with only 20% in the sham group after three years.
Aflibercept provides the broadest therapeutic approach by binding to VEGF-A, VEGF-B, and placental growth factor. The VIVID-DME and VISTA-DME clinical trials showed mean vision improvements of 12.5 and 11.1 letters after two years, compared to merely 0.2 letters with laser treatment.
Bevacizumab offers a cost-effective alternative originally developed for cancer treatment but is used by some ophthalmologists off-label for DME at a lower cost per injection compared to aflibercept and ranibizumab.
The Protocol T clinical trial (conducted by the Diabetic Retinopathy Clinical Research (DRCR) Retina Network) demonstrated that at two years, aflibercept improved vision by 12.8 letters, ranibizumab by 12.3 letters, and bevacizumab by 10.0 letters. However, for patients with worse baseline vision (20/50 or worse), aflibercept showed superior results.
The ophthalmologists at Chang Eye Group in Pittsburgh have extensive experience treating diabetic macular edema and diabetic retinopathy. Schedule an appointment with one of our eye doctors to determine how far the condition has progressed and discuss which treatment options are best for you.
Corticosteroid medications
When anti-VEGF medications alone aren’t sufficient, corticosteroids address inflammation through multiple pathways beyond VEGF blockade. These powerful medications reduce inflammatory cytokines, improve blood-retinal barrier integrity, and decrease vascular permeability. However, these medications can cause serious side effects and should be carefully managed by your eye doctor.
Long-acting steroid implants
For patients requiring sustained treatment, long-acting steroid implants offer extended medication release. The dexamethasone intravitreal implant releases medication for up to six months. The MEAD study found that 22.2% of patients achieved 15-letter improvement or greater, compared to 12% with sham treatment.
The fluocinolone acetonide intravitreal implant provides even longer-lasting relief with sustained release for up to three years. Results from the FAME studies showed that over 28% of patients gained 15 or more letters over three years.
Treatment response and outcomes
Understanding realistic expectations will help you and your eye doctor work effectively with your treatment plan. Response rates vary considerably among patients. DME persisted in about 31-65% of patients despite multiple anti-VEGF injections. Real-world settings reveal additional challenges: 21% of participants experienced decreased vision, and 41% had less than 10% reduction in central macular thickness after 12 months of treatment.
These statistics emphasize the importance of personalized treatment approaches and close monitoring with your eye care specialist to achieve optimal outcomes with your vision.
Injection-Based Diabetic Macular Edema Treatments
How intravitreal injections work
Intravitreal injections might sound unnerving, but these procedures deliver medication precisely where your retina needs it most. The injection targets the vitreous cavity, the jelly-like space in the back of your eye, allowing medication to work directly on damaged blood vessels.
Your comfort matters throughout the entire process. Your eye and eyelids receive anesthetic drops or gel so the injection doesn’t hurt. The eye and eyelids are cleaned using povidone-iodine, a yellow solution that kills bacteria around the eye. An eyelid speculum keeps your eyelids open during the procedure.
You’ll be asked to look in a particular direction while the medicine is injected through the pars plana (the white part of your eye) with a very small needle. Most patients feel pressure with little or no pain during the injection. The entire process typically takes about 10 to 15 minutes.
Injection frequency and scheduling
Your treatment schedule depends on how your eyes respond to medication. Initially, most treatment protocols require monthly injections. The DRCR anti-VEGF treatment plan recommends six monthly injections unless vision reaches 20/20 or better and central subfield thickness normalizes, in which case treatment may be withheld starting at the fourth month. Following the initial phase, eyes showing stability may be followed up in 3-4 months.
Keep in mind that real-world practice often differs from clinical trial protocols. Anti-VEGF frequencies for DME range from 2.2 to 4.4 injections each year in typical practice settings. This contrasts sharply with clinical trials where patients receive an average of 9-12 injections per year!
Managing treatment burden
The time commitment for macular edema treatment extends beyond the injection itself. Each appointment requires an average of an hour to an hour and 20 minutes at your ophthalmologist’s office. When you factor in travel time, each injection appointment can take 2.5 hours of your day. Understanding this time commitment can help you plan your treatment schedule around work, family, and other commitments.
Side effects and safety considerations
Serious complications from intravitreal injections remain extremely rare, with endophthalmitis occurring in less than 0.3% of cases. A recent study of 45,000 eyes found that the total rate of complications was lower than 2%, with most being minor and not requiring medical intervention.
These safety statistics reflect the skill of experienced retina specialists and the refined techniques developed over decades of injection procedures. Your eye care team will monitor you carefully after each injection to ensure your safety and treatment success.
Laser Treatment Options for Macular Edema
ETDRS focal and grid laser photocoagulation
Laser photocoagulation served as the gold standard for DME treatment for three decades before anti-VEGF therapies changed everything. The Early Treatment Diabetic Retinopathy Study (ETDRS) revealed that focal and grid laser reduced moderate vision loss by 50% at three years. These treatments work through two distinct approaches: focal laser targets leaking microaneurysms directly like precision strikes, while grid treatment applies burns spaced two burn widths apart across areas of diffuse edema.
Modern protocols have evolved beyond the original harsh applications. Modified ETDRS approaches use lighter burns at 50 μm spot size instead of the original 50-200 μm range. These gentler applications create gray color changes rather than white burns, dramatically reducing your risk of retinal scarring and vision loss.
Laser treatment does not provide immediate results. It typically takes 2 to 3 months to take effect, and changes may only last a few months. Your ophthalmologist will explain the best treatment options for your specific conditions.
Subthreshold micropulse laser therapy
Another treatment option that may be considered is subthreshold micropulse laser (SML) therapy. This technique delivers energy in carefully timed on and off cycles, allowing tissue cooling between pulses to avoid permanent damage.
Recent research shows that SML provides equivalent outcomes to standard laser for DME when central retinal thickness measures less than 400 μm. The study confirmed that subthreshold micropulse was noninferior to standard laser, with both groups experiencing minimal vision changes at 24 months.
Navigated and image-guided laser systems
Precision is extremely important for laser treatment. The Navilas system uses computer-guided laser delivery with digital imaging, achieving a 92% microaneurysm hit rate compared to 72% with conventional manual laser techniques. The system works by automatically positioning and stabilizing the aiming beam during treatment. This remarkable precision reduced retreatment rates by almost half.
When laser treatment is recommended
Your doctor may recommend laser as first-line therapy for non-center-involving clinically significant macular edema and when you decline injections. For center-involving DME, laser becomes a second-line treatment after four to six anti-VEGF injections show incomplete response.
Your ophthalmologist will evaluate laser therapy options based not only on your eye conditions including retinal thickness, but also on the type of laser machines available for your treatment.
Advanced Treatment Strategies that Reduce your Treatment Burden
Your treatment plan doesn’t have to rely on a single approach. Modern macular edema management often combines different therapies to maximize vision improvement while reducing the frequency of appointments and procedures you need.
Laser plus anti-VEGF therapy
Combining subthreshold micropulse laser (SML) with anti-VEGF therapy creates superior outcomes for specific patient groups. Studies demonstrate the combined approach produces greater LogMAR visual acuity improvements at 6 and 12 months, particularly when baseline central macular thickness measures under 400 μm.
The results speak for themselves: the READ-2 study found ranibizumab monotherapy required 9.3 injections over two years, whereas combination therapy with focal/grid laser needed only 2.9 injections. This dramatic reduction in injection frequency means fewer clinic visits, less time away from work, and reduced treatment burden for you.
Reducing injection frequency with strategic combinations
Advanced laser systems offer even greater advantages when combined with anti-VEGF therapy. The Navilas navigated laser system combined with ranibizumab produced similar visual outcomes to monotherapy but required significantly fewer injections after the loading phase: 0.88 versus 3.88 injections. This effect lasted 36 months for study patients.
Anti-VEGF medications combined with corticosteroids demonstrated advantages within three months of treatment. However, combination therapy carries higher risks of elevated intraocular pressure and cataract progression. Your eye doctor will carefully monitor these potential complications to ensure your treatment remains both safe and effective.
Precision treatment through advanced imaging
Spectral domain optical coherence tomography (SD-OCT) is another essential tool for managing diabetic macular edema. Your doctor can now combine multiple imaging techniques to create detailed treatment maps that guide precise therapy decisions. Machine learning also continues to advance and may soon provide treatment algorithms based on multimodal imaging, providing even more personalization to your care.
Breakthrough therapies on the horizon
Faricimab represents a new generation of treatment, combining anti-VEGF and angiopoietin-2 properties to offer hope for patients who haven’t responded well to standard therapy. Natural-derived compounds can also enhance conventional therapies including intravitreal injections and laser treatment.
These emerging options mean that even if initial treatments don’t provide optimal results, additional effective alternatives continue to become available. The eye doctors in Pittsburgh at Chang Eye Group continually monitor and implement these advances for treating diabetic macular edema and diabetic retinopathy. Schedule an appointment at one of our Pittsburgh locations to evaluate your condition and explore your treatment options.
Protecting Your Vision from Macular Edema
Macular edema treatment has transformed dramatically over the past decade. Anti-VEGF injections now deliver superior outcomes compared to laser therapy alone, offering hope for patients who once faced inevitable vision loss. While the treatment journey requires commitment and regular appointments, strategic combination approaches can significantly reduce your injection burden without compromising results.
Your response to treatment depends on many factors unique to your condition. Working closely with your retina specialist ensures you receive the most effective protocol tailored specifically to your needs. Some patients achieve excellent results with standard approaches, while others benefit from innovative combination therapies that merge the precision of modern laser techniques with the power of anti-VEGF medications.
Early intervention makes the difference between preserving your sight and losing it. Response rates vary among patients, but one factor remains constant across all treatment approaches: timing matters. The sooner you begin appropriate treatment, the better your chances of maintaining clear vision for years to come. Don’t wait for symptoms to worsen or hope the condition will resolve on its own.
Your vision deserves expert care from specialists who understand the full spectrum of treatment options available today. Whether you’re facing initial treatment decisions or seeking better management of persistent macular edema, Chang Eye Group in Pittsburgh provides the advanced care and personalized approach you need.
Schedule your eye exam today at Chang Eye Group to discuss which treatment strategy offers the best protection for your specific condition and prevents further vision loss.
FAQs
Q: What are the most effective injection medications for treating macular edema?
A: Anti-VEGF medications like ranibizumab, aflibercept, and bevacizumab are the most effective first-line treatments for macular edema. These injections work by blocking vascular endothelial growth factor, which reduces fluid leakage and swelling in the macula. Studies show that 40-44% of patients receiving these treatments experience significant vision improvement.
Q: Is laser treatment still a viable option for macular edema?
A: Yes, laser treatment remains an important option for macular edema, though it’s no longer the primary first-line therapy. Focal and grid laser photocoagulation can reduce moderate vision loss by 50% at three years. It’s particularly recommended for non-center-involving macular edema and as a second-line treatment when anti-VEGF injections show incomplete response after four to six treatments.
Q: How often do patients need to receive anti-VEGF injections?
A: Most treatment protocols initially require monthly injections for the first six months. After this loading phase, injection frequency may be reduced based on individual response. In real-world practice, patients typically receive between 2-5 injections per year, though clinical trials often involve 9 to 12 injections annually for optimal results.
Q: Can combining laser therapy with injections reduce treatment burden?
A: Yes, combining subthreshold micropulse laser with anti-VEGF therapy can significantly reduce the number of required injections. Studies show that combination therapy requires only 2.9 injections over two years compared to 9.3 injections with anti-VEGF alone, while maintaining similar visual outcomes. This approach is particularly effective for patients with baseline central macular thickness under 400 μm.
Q: How long does medication from an eye injection remain effective in the body?
A: Anti-VEGF medications typically remain in your system for about 1 to 2 months after injection, which is why monthly treatments are often recommended initially. Newer formulations like Eylea HD contain higher doses and can last longer, allowing for extended intervals between injections while maintaining therapeutic effectiveness.